





Background
A 60-year-old male, presented with neck pain, giddiness, vomiting, imbalance since 2-3 weeks. MRI brain with contrast showed left cerebellar lesion extending to cervico-medullary junction with compression. Biopsy sent for examination.
Microscopy
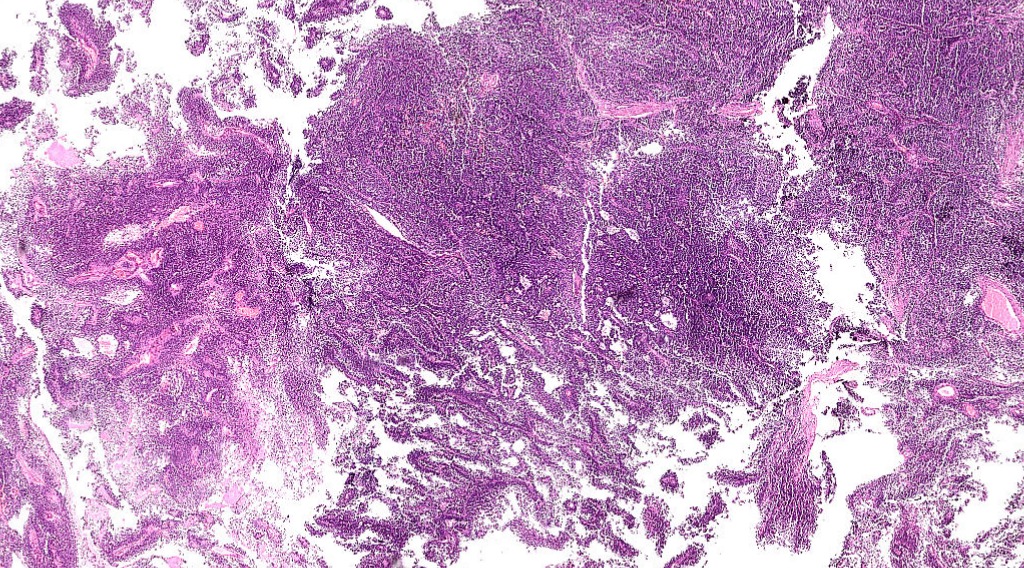
Fig.7a; H&E; 1.25x
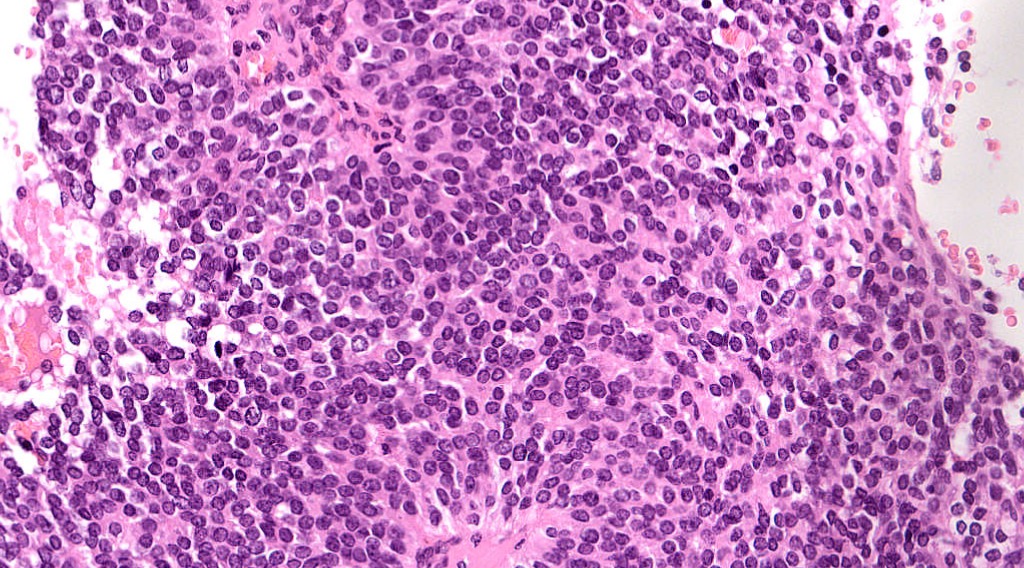
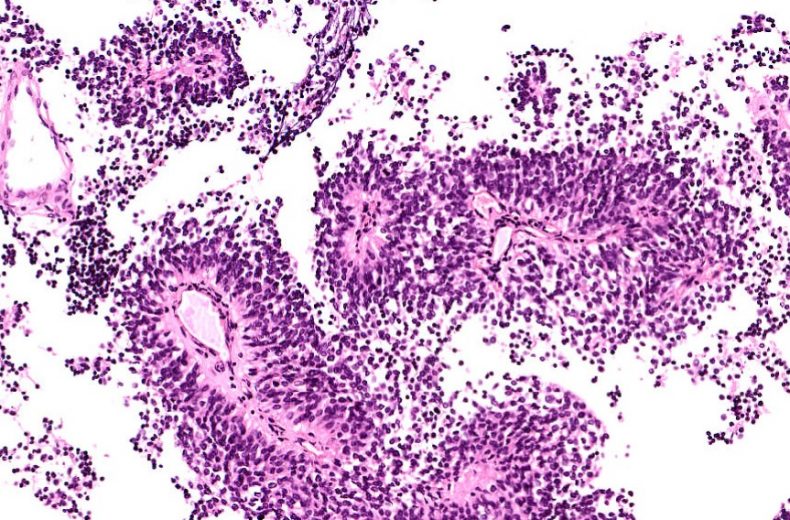
Fig.7b; H&E; 20x
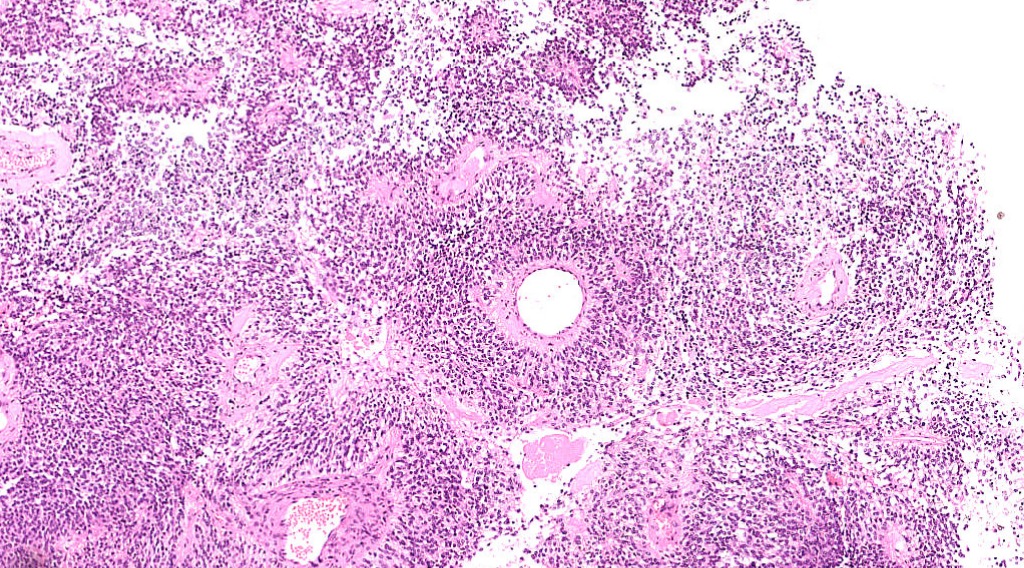
Fig.7c; H&E; 5x
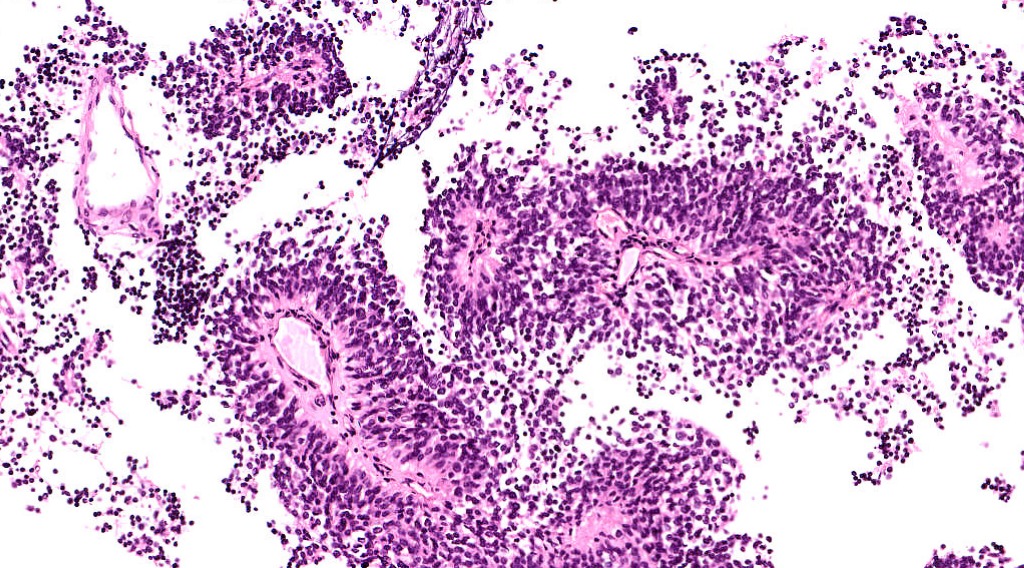
Fig.7d; H&E; 10x
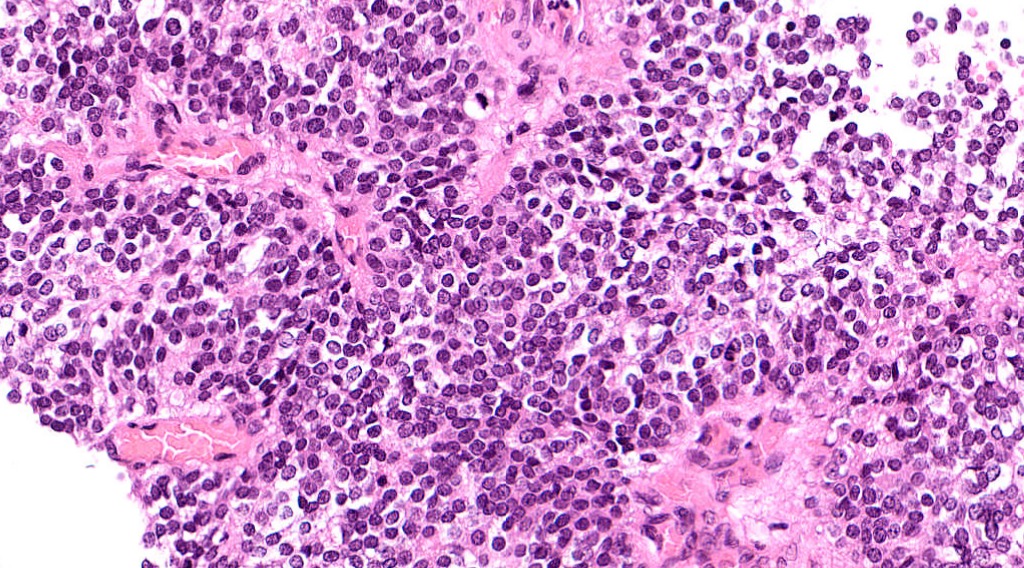
Fig.7e; H&E; 20x
Images show a cellular tumor composed of monomorphic tumor cells arranged in papillary and perivascular pseudorosettes [Fig.7a-7d]. There is abundant vascular proliferation with increased mitotic activity [Fig.7e]. No evidence of necrosis is seen.
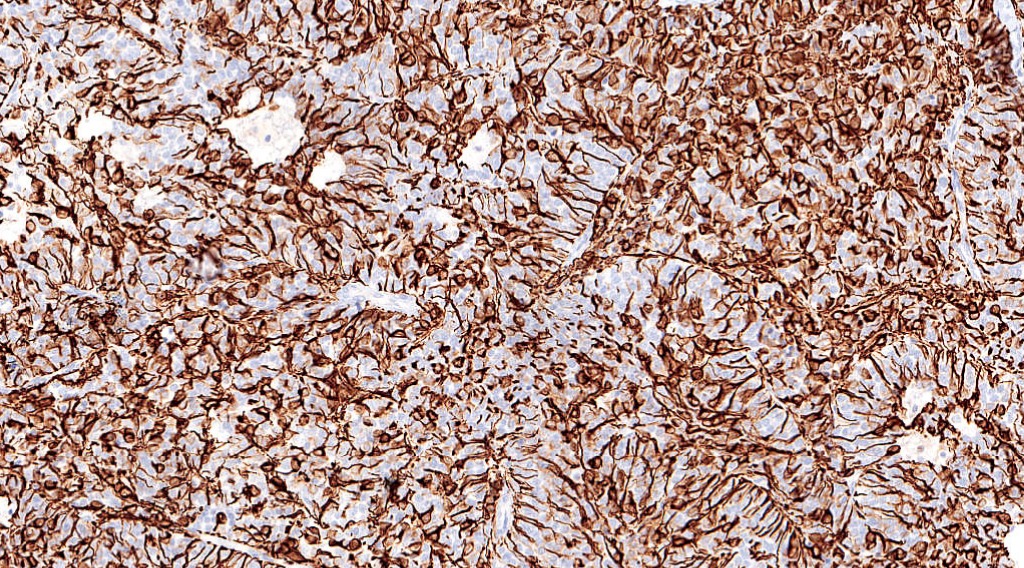
Fig.7f; GFAP
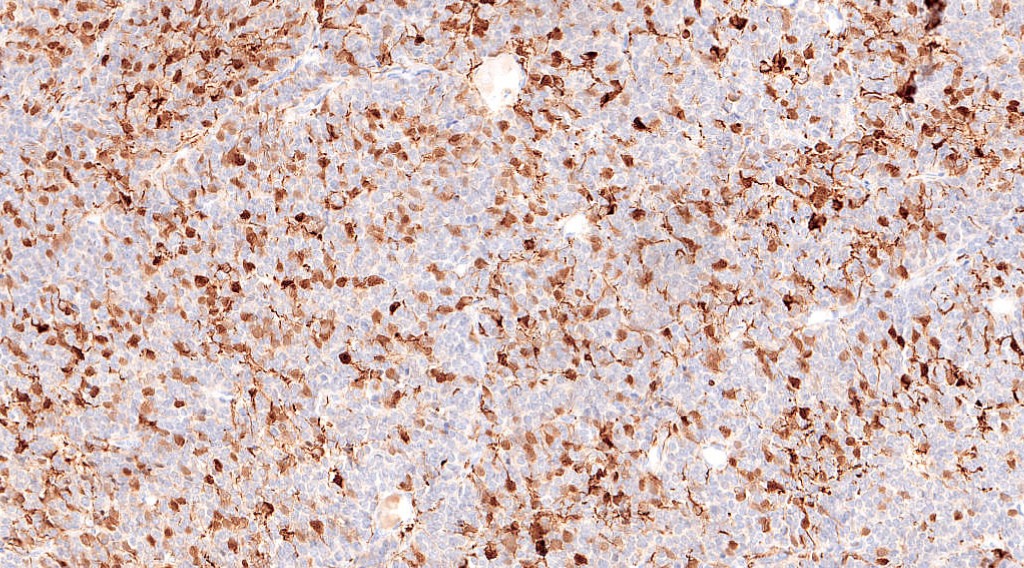
Fig.7g; s100
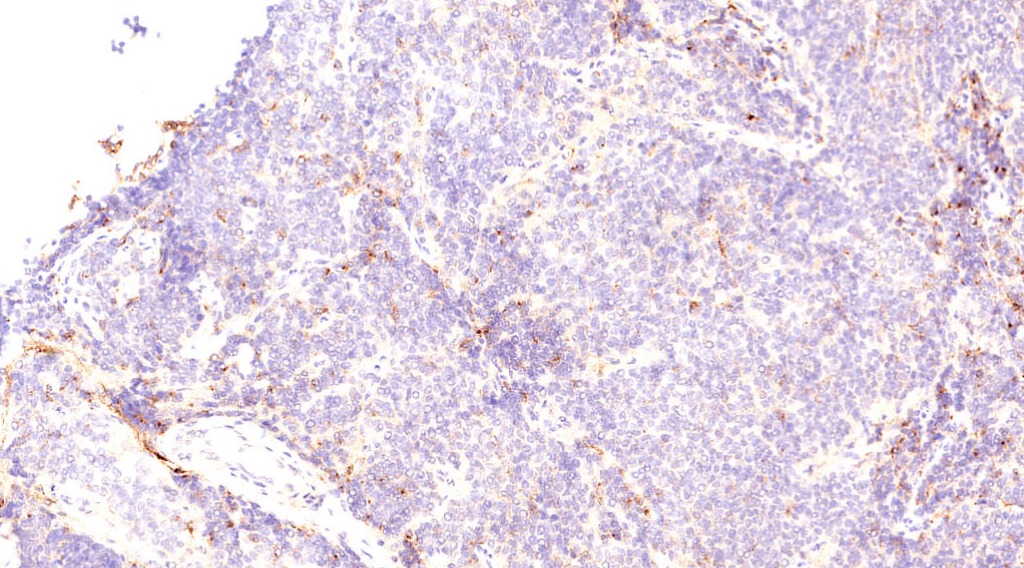
Fig.7h; EMA
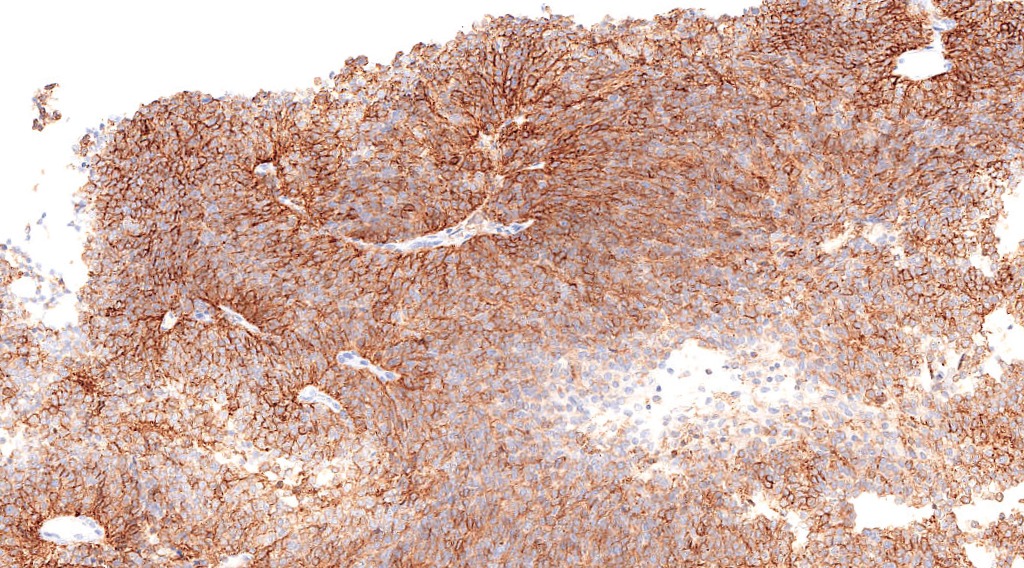
Fig.7i; L1CAM
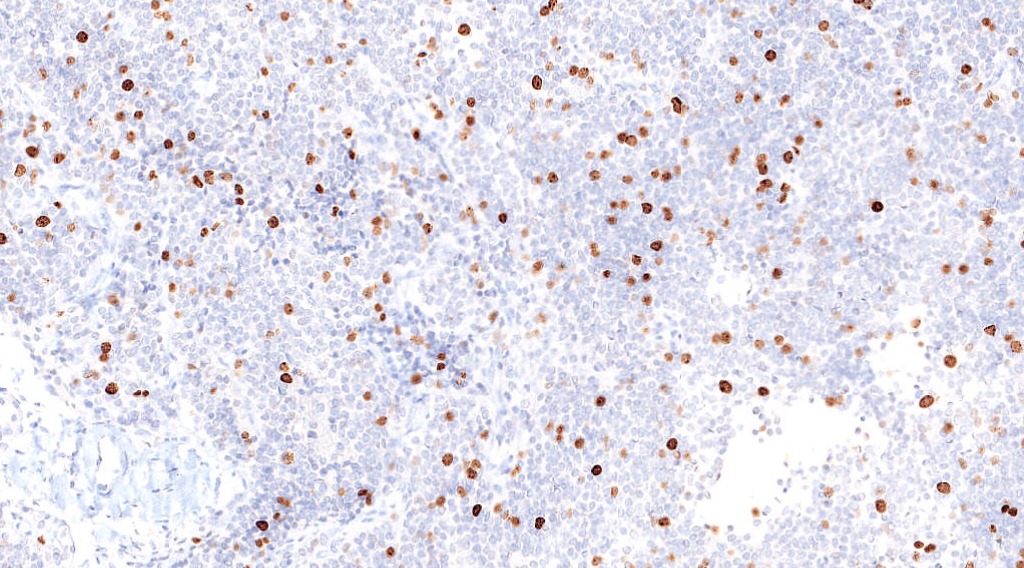
Fig.7j; Ki67
On Immunohistochemistry, tumor cells were positive for GFAP, s100 & EMA(dot-like) [Fig.7f-7h]. Strong L1CAM expression was noted [Fig.7i]. Ki67 mitotic index was 30-40% [Fig.7j].
Final Impression: Anaplastic Ependymoma- CNS WHO Grade 3.
- Location:
- Pediatric: intracranial, posterior fossa
- Adults: spinal cord
- Associated with NF2
- 3 variants: Papillary, clear cell and tanycytic
- Features of Anaplasia: increased cellularity, high N:C ratio, nuclear pleomorphism, increased mitosis & prominent microvascular hyperplasia.
- RELA fusion positive ependymoma:
- 70% pediatric supratentorial tumors
- C11orf95(ZFTA)-RELA fusion gene involving chr 11
- L1CAM protein expression correlates well with presence of RELA fusion gene
- Poor prognosis
- Myxopapillary ependymoma:
- Cauda equina region in adults
- CNS WHO Grade 1
- Biologically benign but local recurrence and CSF dissemination common
- Favourable prognosis
- Immunohistochemistry:
- Positive stains: GFAP, S-100, vimentin, EMA
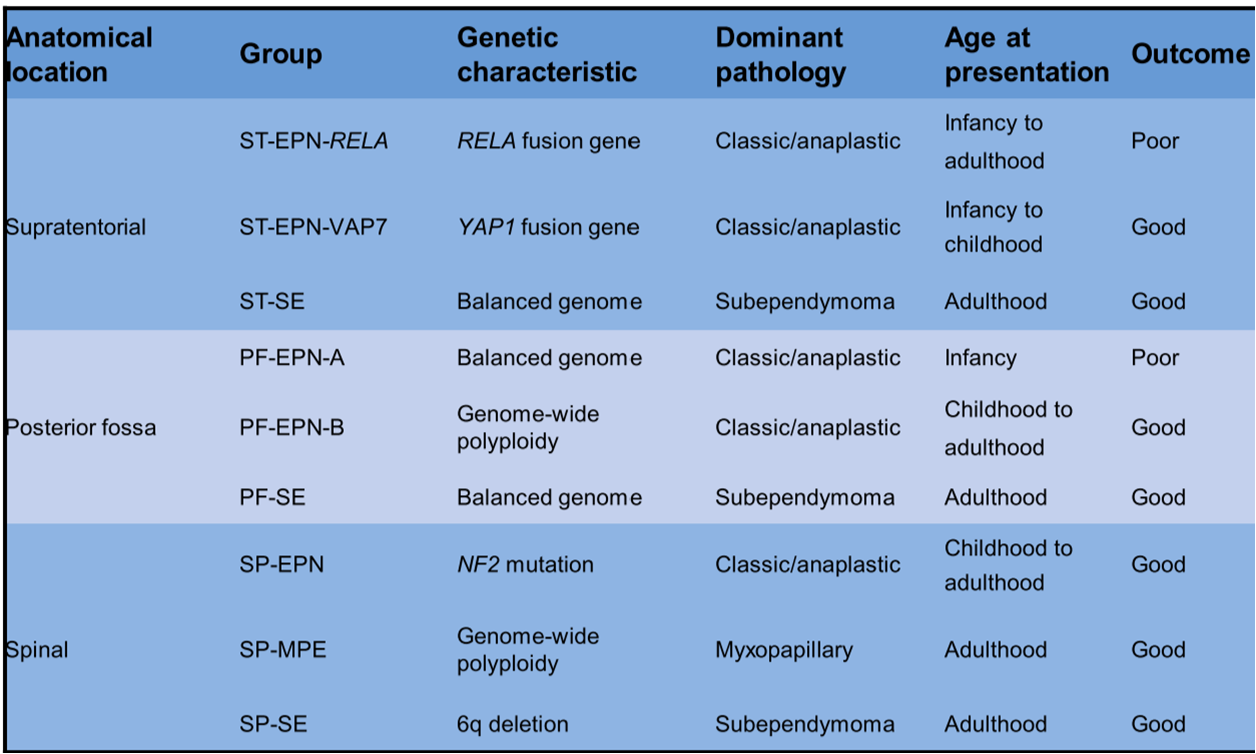
- Molecular subgroups of ependymoma:
*Note: The terminology and criteria used are in line with the current WHO CNS (2016) classification, which may change in the upcoming edition(s).
Contributed by: Dr. Garima Durga
Compiled by: Dr. Ankur Kumar & Dr. Himanshi Diwan
In case of queries, email us at: kumar.ankur@rgcirc.org
Anaplastic ependymoma Central nervous system Ependymoma
Last modified: 05/06/2021