





Background
A 51-year-old hypertensive lady with recently diagnosed Diabetes mellitus, presented with complaints of weight gain and hair loss. CT whole abdomen showed a large soft tissue lesion in right supra renal region measuring 8 x 6cm. Serum cortisol: 39.26 mcg/dl. Surgical excision was performed.
Gross specimen

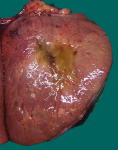
Fig. 16a; Gross 1: A circumscribed bright yellow to orange coloured tumor

Fig. 16b; Gross 2: Tumor with myxoid areas
Microscopy
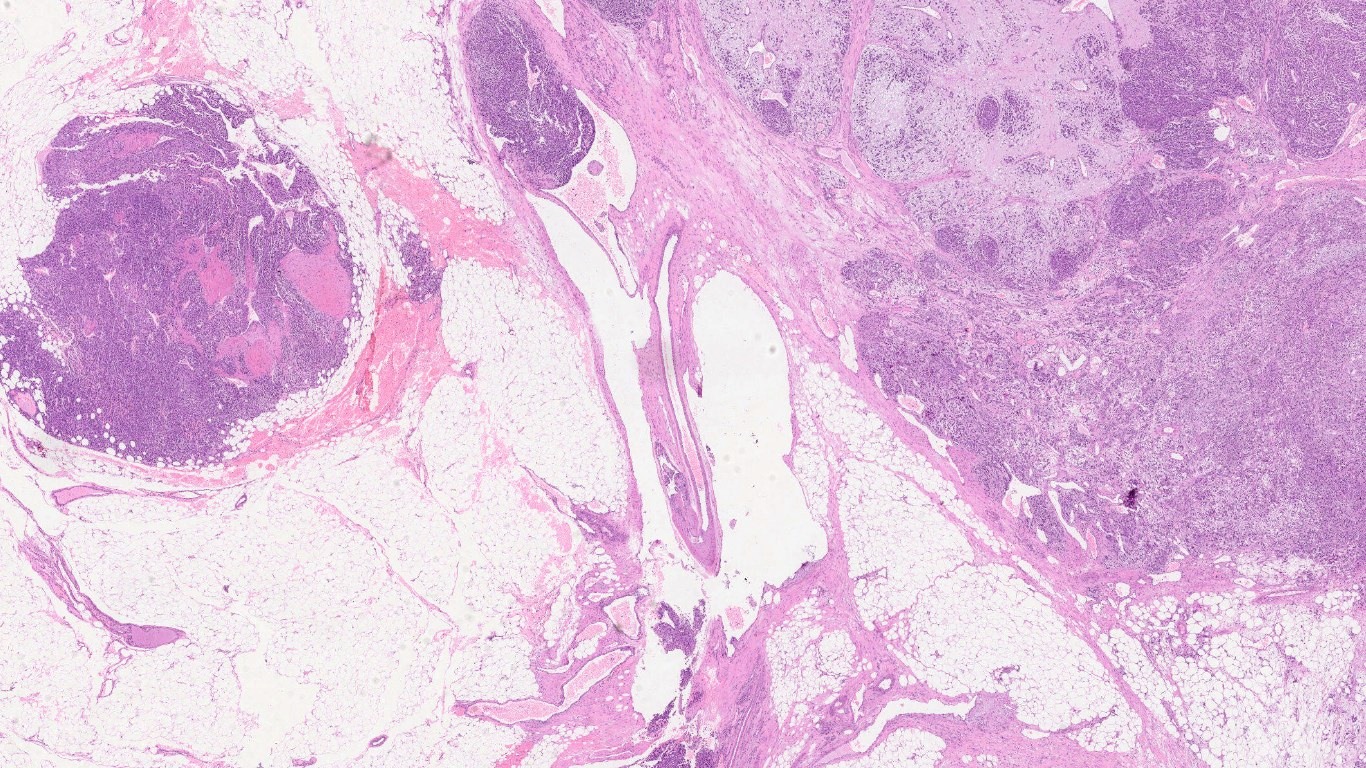
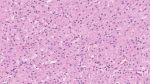
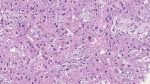
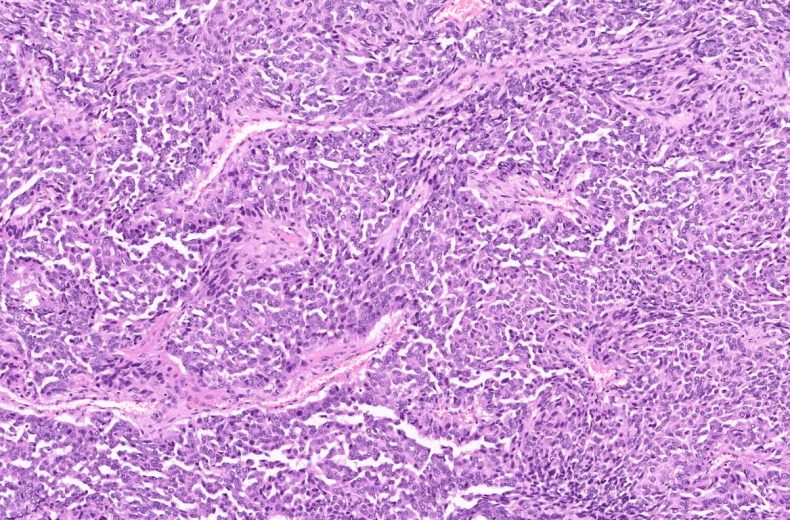
Fig 16c; H&E; 4x
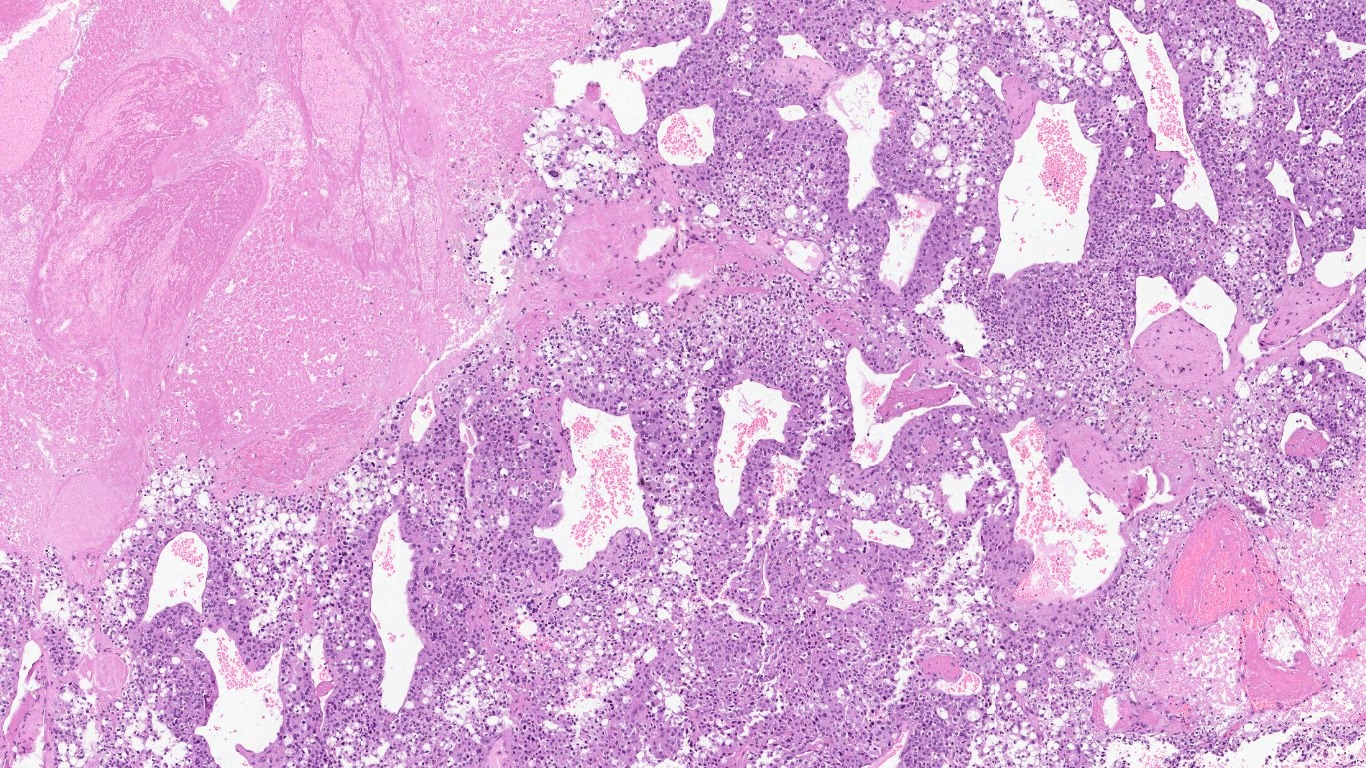
Fig 16d; H&E; 10x
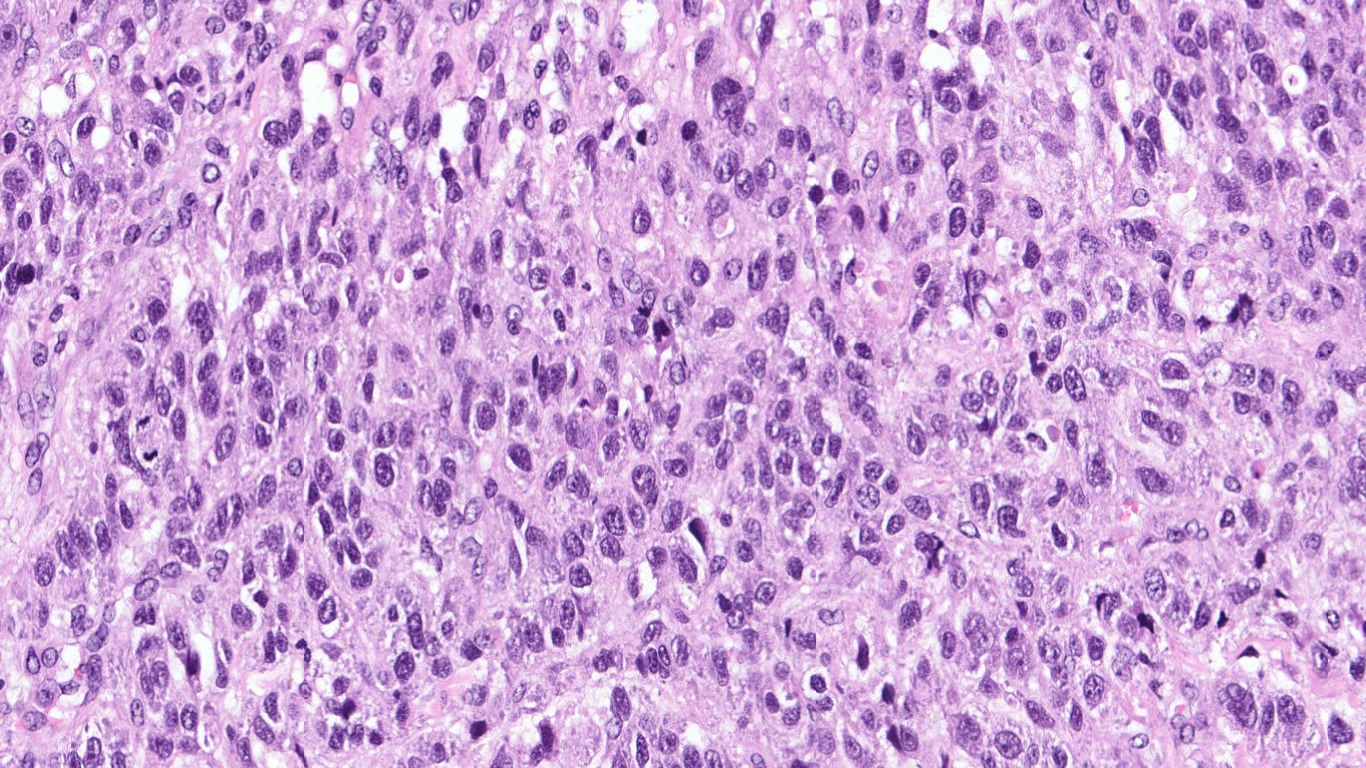
Fig 16e; H&E; 20x

Fig 16f; H&E; 40x
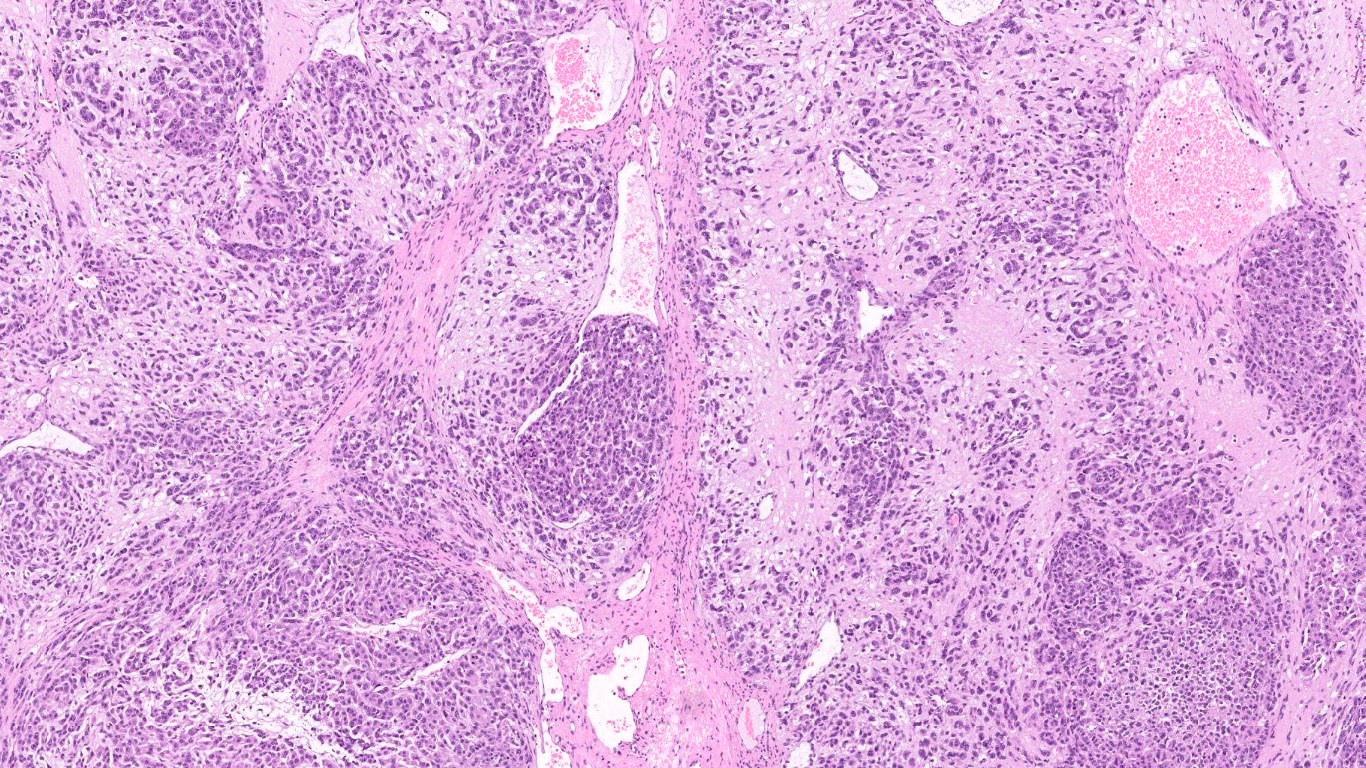
Fig 16g; H&E; 10x
Immunohistochemistry
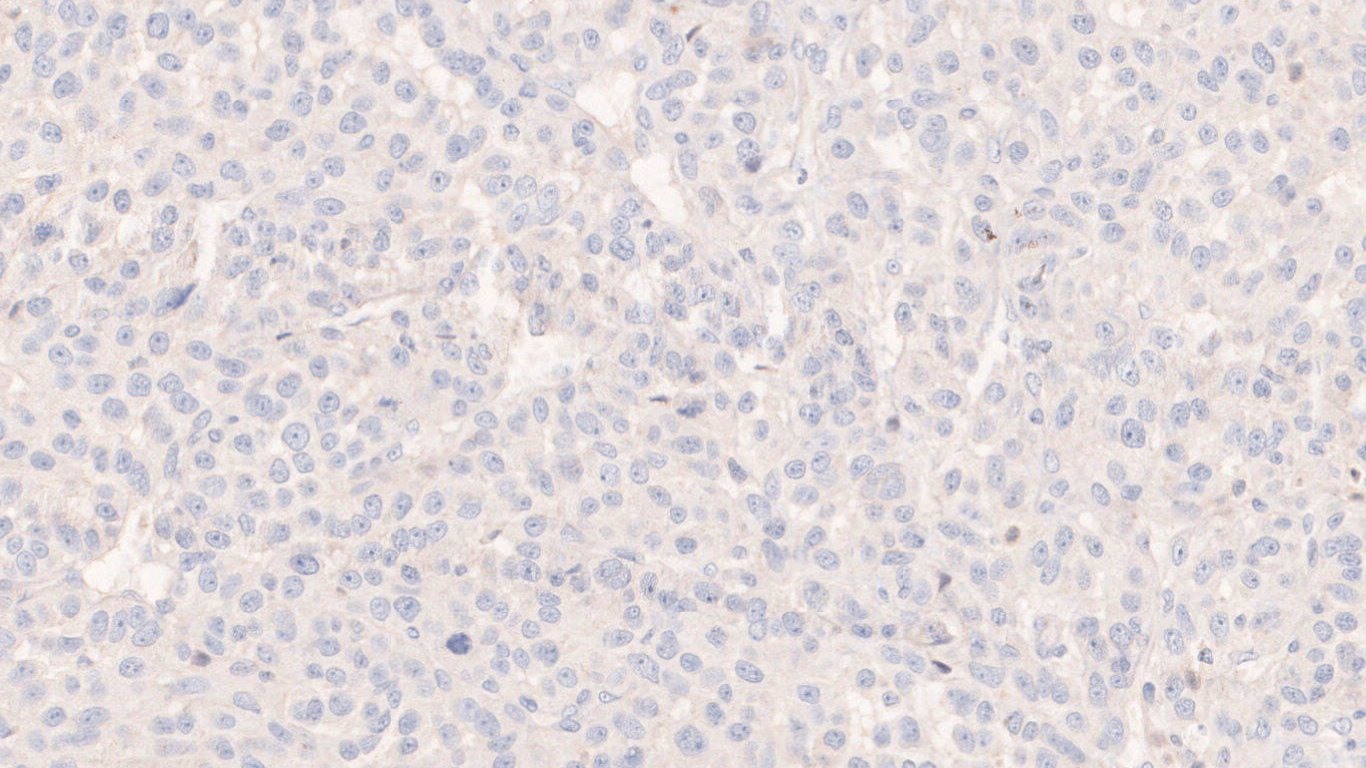
Fig 16h; CK

Fig 16i; Chromogranin A
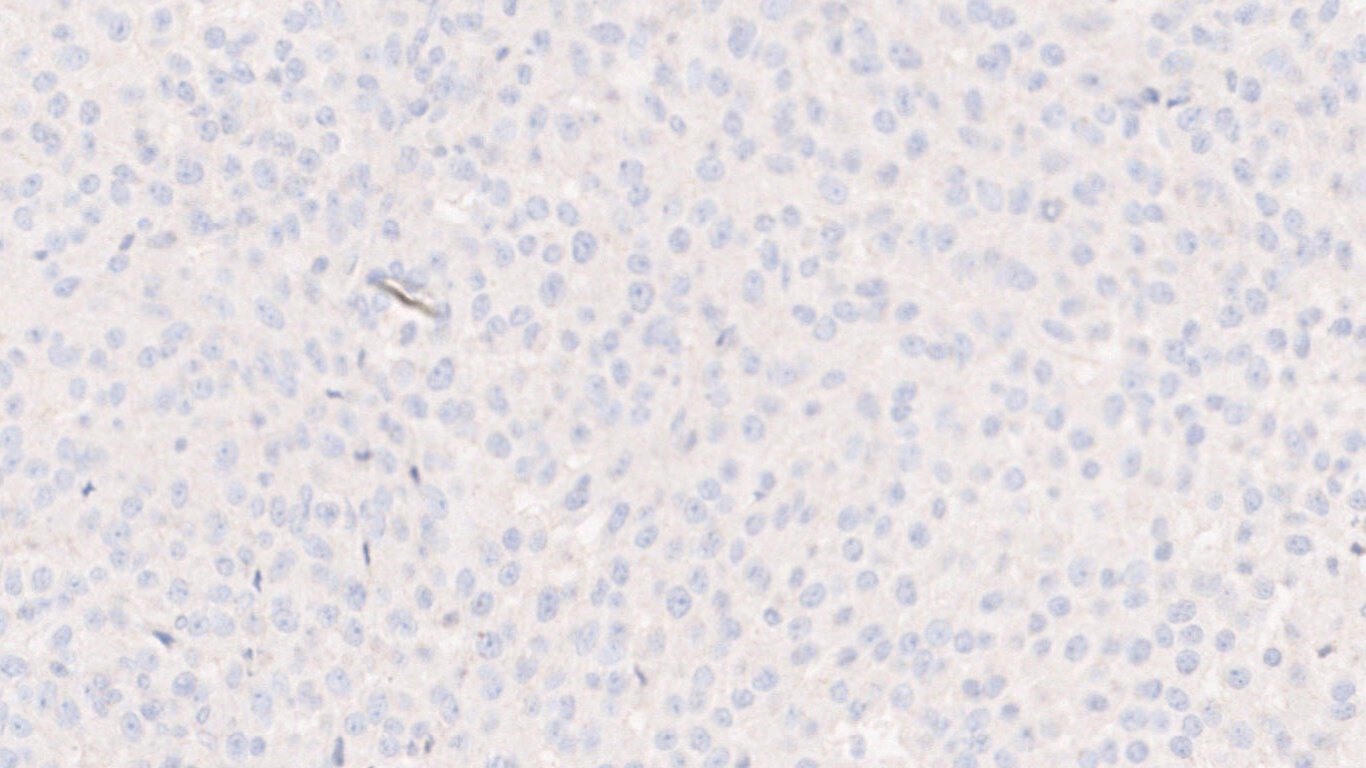
Fig 16j; PAX-8
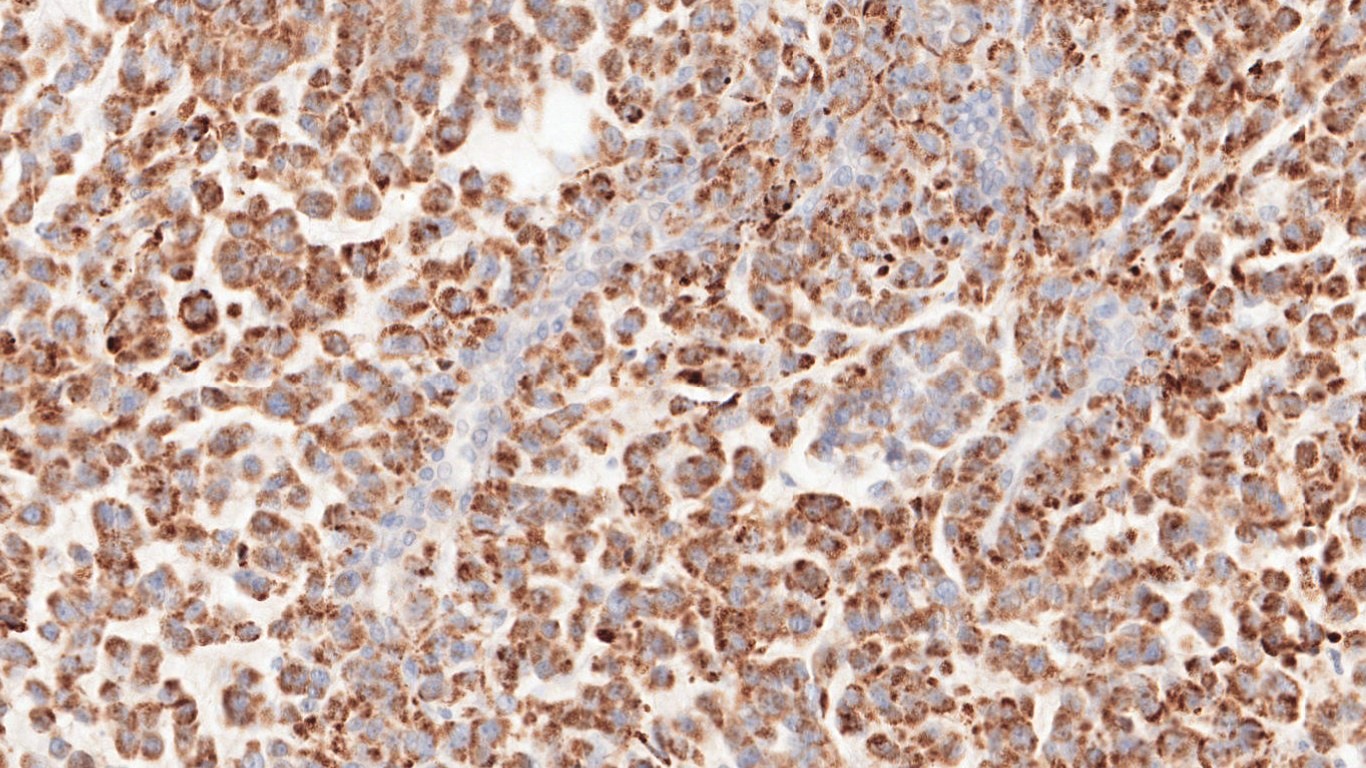
Fig. 16k; Melan-A
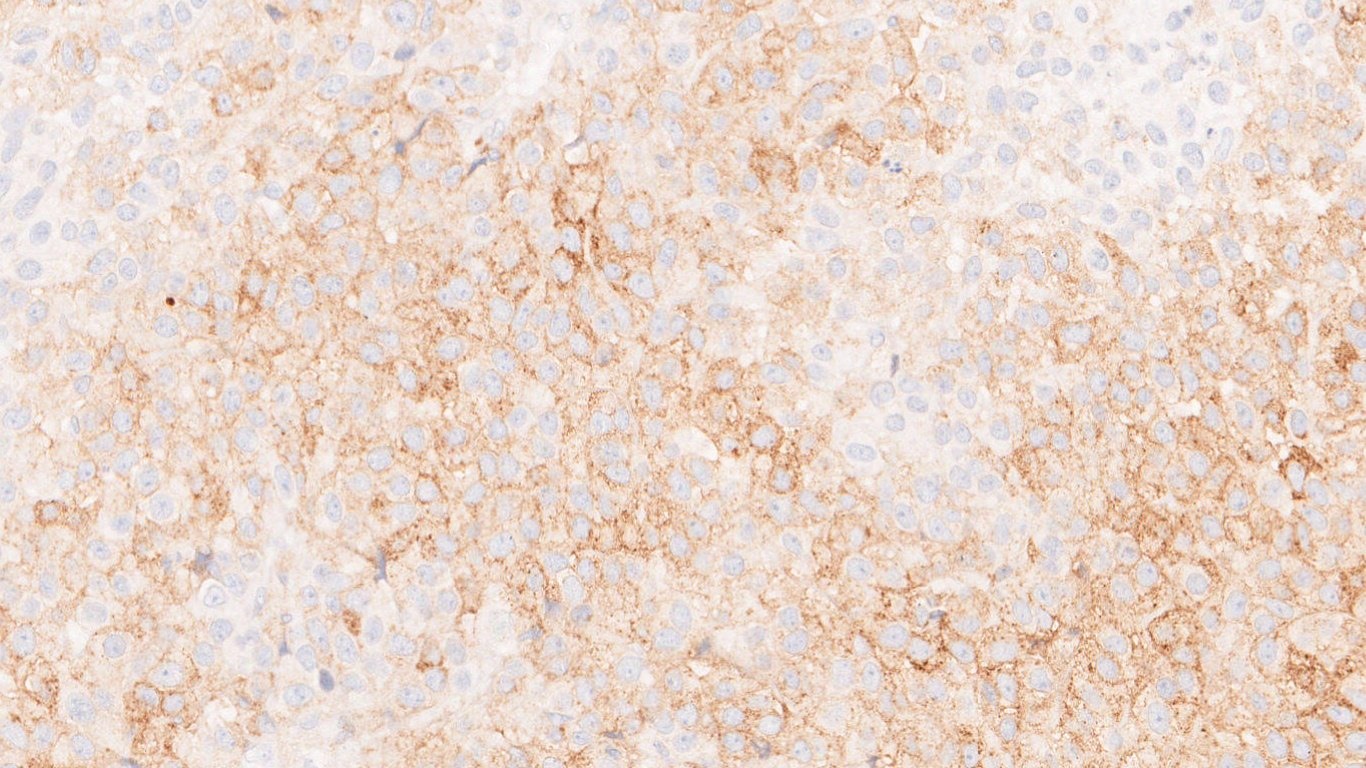
Fig 16l; Synaptophysin
Questions & Answers:
- What is your diagnosis?
- Adrenal cortical adenoma
- Adrenal cortical carcinoma –low grade
- Adrenal cortical carcinoma –high grade
- Pheochromocytoma
- Which of the following is/are associated with this tumor?
- Li Fraumeni syndrome
- Beckwith-Wiedemann syndrome
- Congenital adrenal hyperplasia
- All of the above
- Definitive criteria for malignancy in this tumor is:
- Distant metastases
- Presence of atypical mitotic figures
- Necrosis
- Vascular invasion
- Which of the following IHC marker is usually not expressed in this tumor?
- Synaptophysin
- Chromogranin A
- Melan A
- Inhibin A
- Malignant epithelial tumor of adrenal cortical cells.
- Median age of presentation: Bimodal, with peaks in 1st and 5th decade of life.
- Female predilection
- Mostly involves single adrenal gland
- If bilateral adrenal enlargement is seen : Think of something else
- Clinical features:
- Symptoms of steroid hormone excess
- Abdominal pain and fullness
- Incidental
- Both androgen and estrogen production in an adrenal tumor: suspicious for adrenocortical carcinoma
- Modified Weiss criteria:
- Score: 2x mitotic rate criterion + 2x clear cytoplasm criterion + abnormal mitosis criterion + necrosis criterion + capsular invasion criterion
- Score ≥3- suggests malignancy
MorphologicalCharacteristics |
Score |
|
Present |
Absent |
|
Mitosis. 5/50 hpf |
1 |
0 |
Clear cells ≤ 25% |
1 |
0 |
Abnormal mitosis |
1 |
0 |
Necrosis |
1 |
0 |
Capsular invasion |
1 |
0 |
- Histological variants:
- Oncocytic
- Myxoid
- Sarcomatoid
- Differential diagnosis:
- Adrenal cortical adenoma
- Oncocytoma
- Pheochromocytoma
- Renal cell carcinoma(primary and metastatic)
- Hepatocellular carcinoma(primary and metastatic)
- Metastatic melanoma
- Immunohistochemistry markers :
- Positive markers: SF-1, Inhibin A , Melan A, Synaptophysin, Calretinin
- Negative markers: CK, EMA & CEA, Chromogranin A(usually negative)
- Reticulin stain: highlights loss of nested architecture
- Genetic alterations:
- Overexpression of IGF2, DLGAP5 & PINK1
- TP53 mutation
- WNT pathway defects (CTNNB1 mutation)
- Associated hereditary syndromes:
- Li-Fraumeni syndrome
- Lynch syndrome
- Multiple endocrine neoplasia type 1
- Familial adenomatous polyposis
- Carney complex
- Beckwith-Wiedemann syndrome
- Neurofibromatosis type 1
- Treatment:
- Surgical excision
- Locoregional lymph node dissection for localized tumor
- Radiation therapy for metastatic tumor
- Adverse prognostic factors:
- Hypercortisolism
- Age>50 years
- Ki67 index-high
- Increased expression of SF-1
Contributed by: Dr. Sunil Pasricha
Compiled by: Dr. Vidya Menon
In case of queries, email us at: info.pathbliss@rgcirc.org
Adrenal Adrenocortical carcinoma Endocrine Neoplasms Weiss criteria
Last modified: 17/08/2021