





Background
11 year old girl, presented with history of transfusion requiring anemia for 3 years. No Organomegaly/ lymphadenopathy seen. No significant family history. CBC reveals Hemoglobin: 6.1 gm/dl, WBC count: 4900 /cumm and platelet count is 3.5 lakh /cumm. MCV is 75.2 fl, MCH is 21.1 pg, RDW CV is 34.1. Corrected retic count on supra vital dye is 0.9. LDH levels are normal. Peripheral smear & Bone marrow aspirate sent for examination.
Microscopy
On peripheral smear, dimorphic blood picture was seen showing two separate populations of microcytic and normocytic red cells. [Fig.5a].
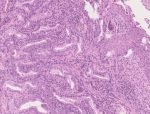
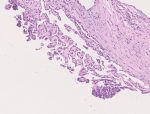
Bone marrow aspirate showed normoblastic erythroid hyperplasia. No significant abnormality in myeloid series seen. [Fig.5b & c]
Prussian blue stain showed numerous ring sideroblasts. Ring sideroblasts showed 5 or more perinuclear iron granules covering atleast 1/3rd nuclear circumference. [Fig.5d]
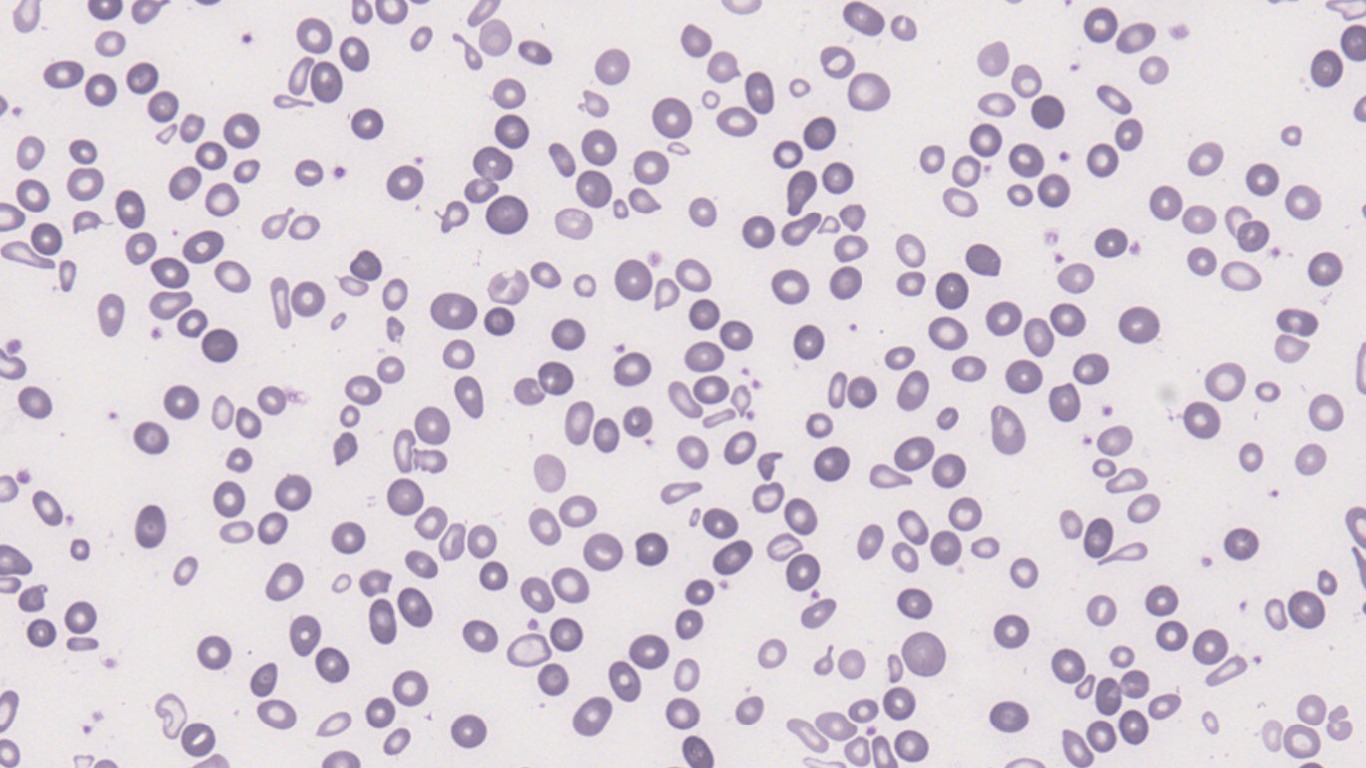
Fig.5a; Peripheral smear; 40x
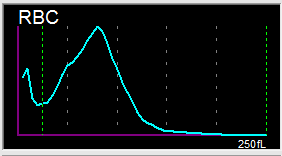
Histogram shows dimorphic RBC population
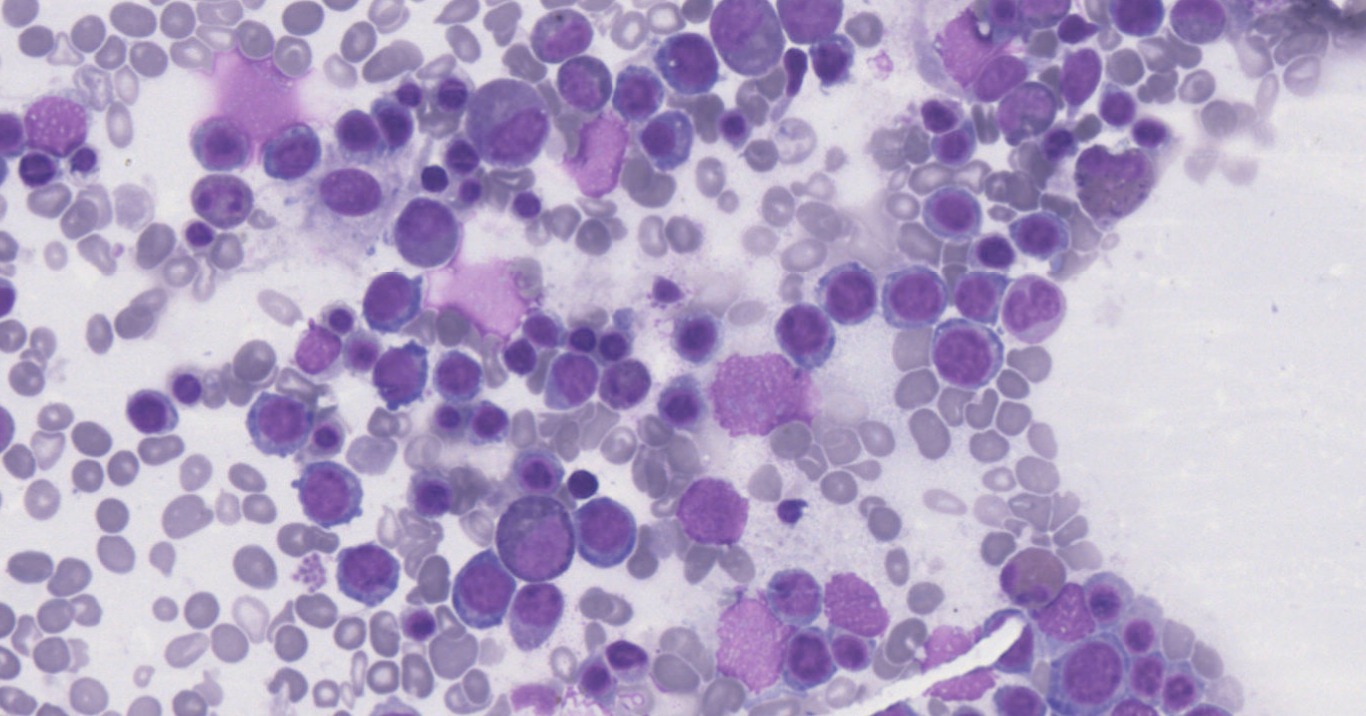
Fig.5b; Bone marrow aspirate; 40x
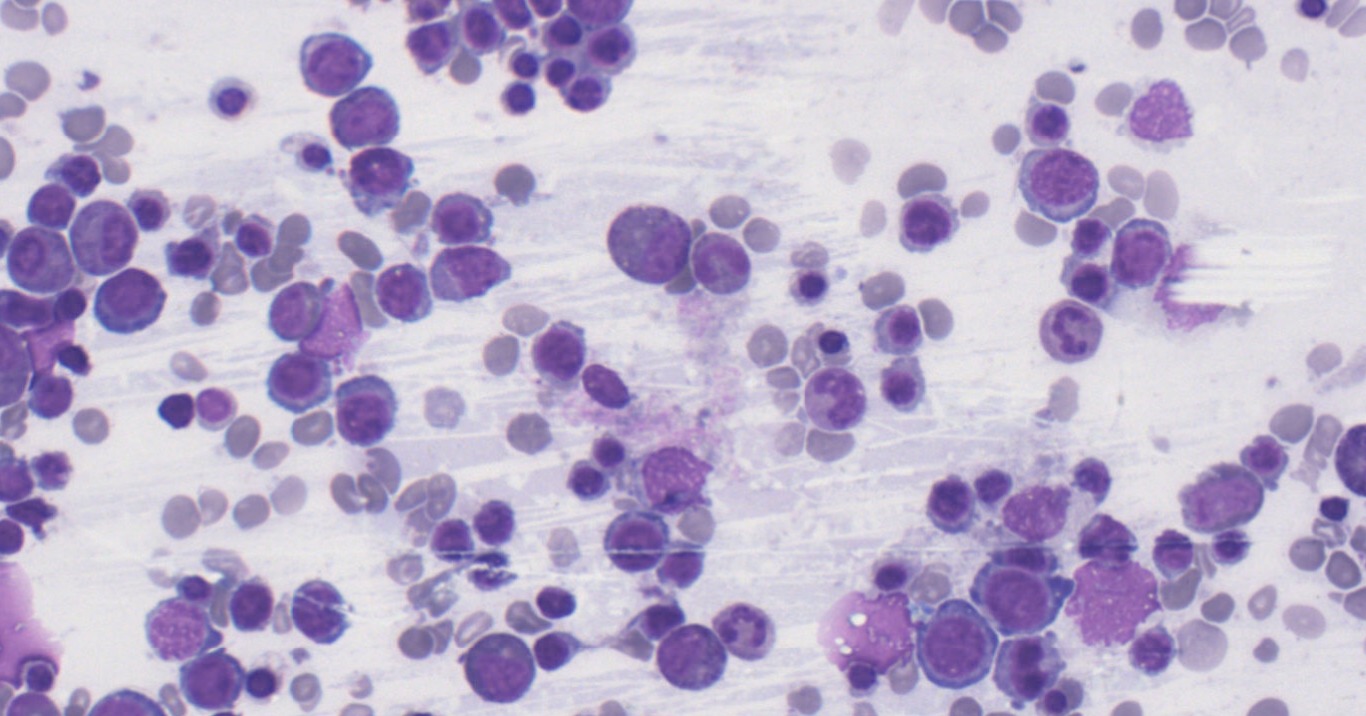
Fig.5c; Bone marrow aspirate; 40x
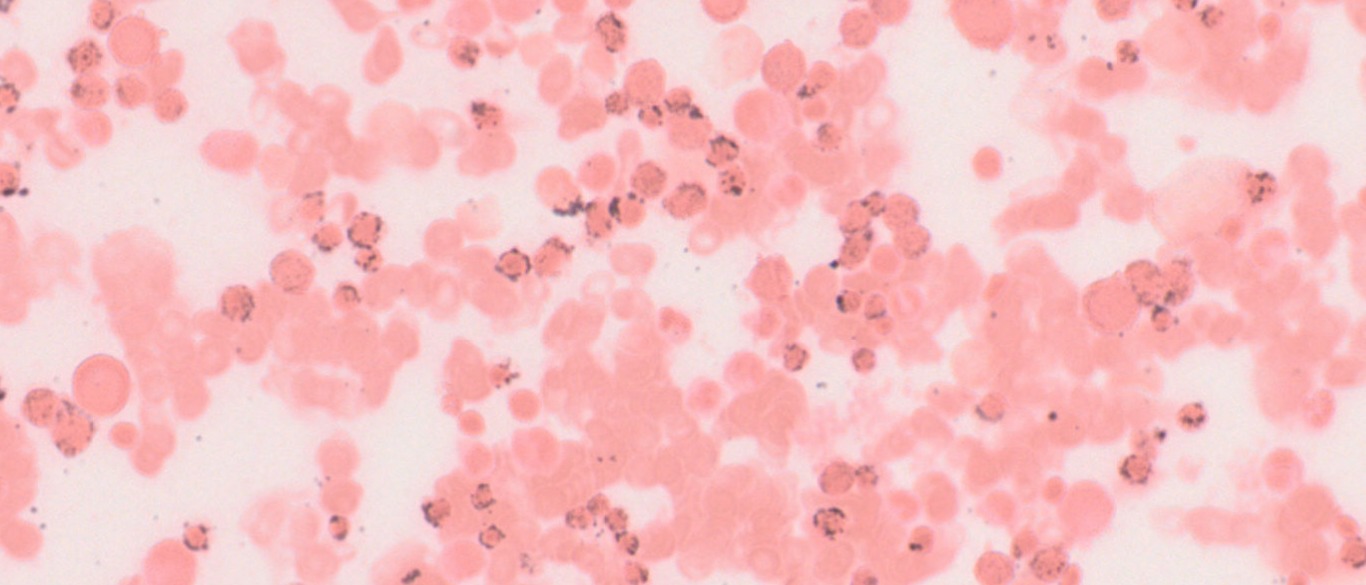
Fig.5d; Perls Prussian Blue; 40x
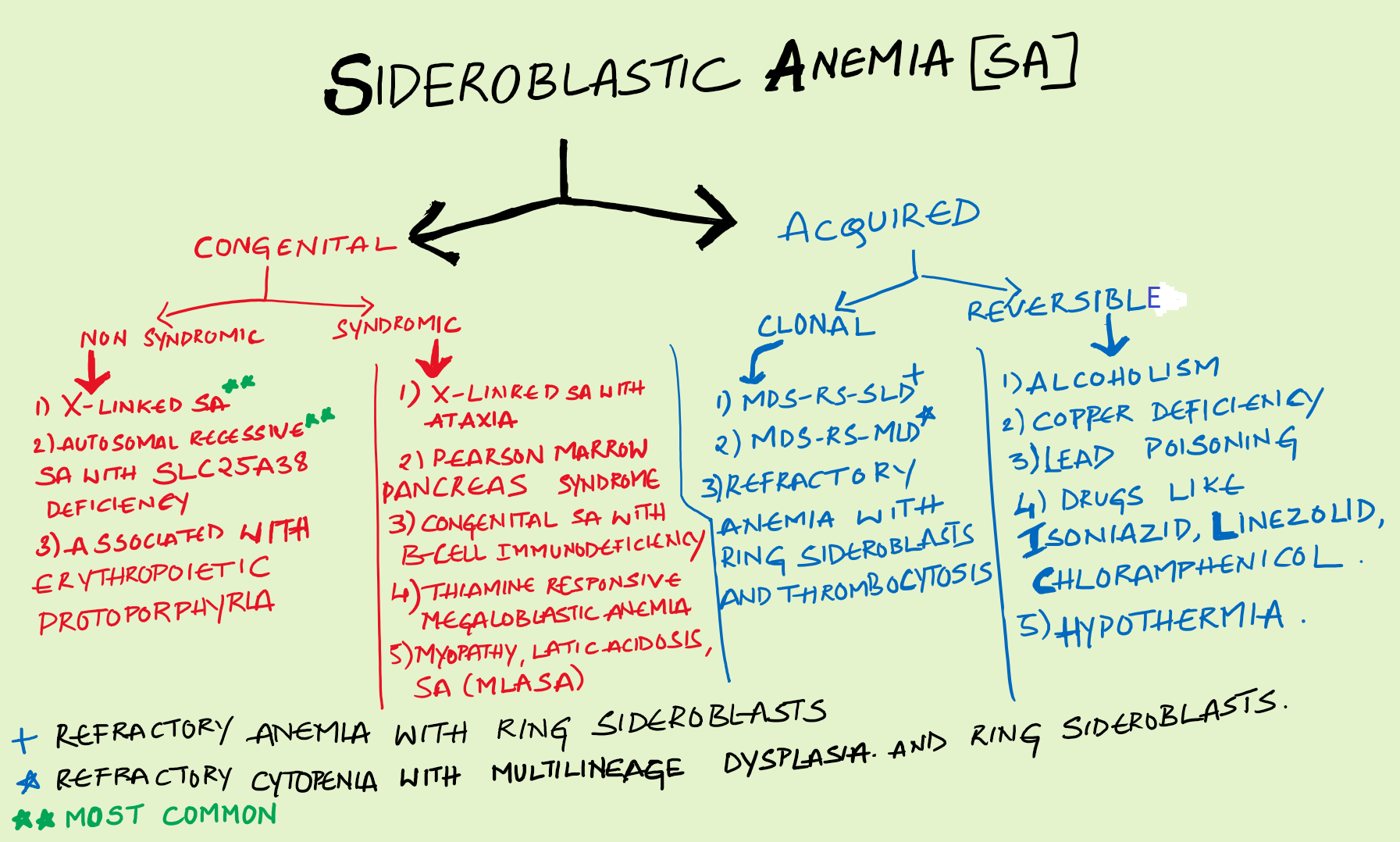
Final Impression: Sideroblastic Anemia.
- Sideroblastic Anemia is characterised by pathological iron deposits in the erythroblast mitochondria in bone marrow (seen as ring sideroblasts).
- Red cell histogram in inherited cases is characterized by dual peak of normocytic and microcytic red cells in absence of transfusion history.
- Multiple pathological processes at the end culminate in a common point leading to imbalance between mitochondrial iron import and its utilization in erythroblasts. (Majority of the cases have an underlying pathology in heme biosynthesis, primarily caused by mutations in ALAS2[5- aminolevulinate synthase] enzyme).
- Clinically presents with variable degree of anemia. Age of presentation and degree of anemia depends on the underlying cause. Congential variants presenting in infancy and early childhood.
- Peripheral smear findings include microcytic hypochromic anemia with dimorphism, Wide RDW, Pappenheimer bodies and siderocytes. Few cases may show normocytic anemia and macrocytic anemia.
- Bone marrow shows normoblastic erythroid hyperplasia with ragged cytoplasmic borders. Increased iron in macrophages and ring sideroblasts on prussian blue stain (characteristic pathological feature is presence of ring sideroblasts)
- Serum ferritin levels are increased with increase in transferrin saturation.
- Treatment includes pyridoxine supplements. Chronic and non responsive cases might need transfusions. Multiple transfusions might lead to Iron over-load and its complications. Few cases might need hematopoeitic stem cell transplantation depending on etiology and clinical response to pyridoxine and transfusions.
Compiled by: Dr. Pratyusha Gudapati & Dr. Namrata Kaul
In case of queries, email us at: kumar.ankur@rgcirc.org
Dimorphic anemia Non neoplastic Prussian blue stain Ring sideroblasts Sideroblastic anemia
Last modified: 05/06/2021